Medical Student Albany Medical College Summerville, South Carolina, United States
Disclosure(s):
Jaclyn Preece, MD: No relevant relationships to disclose.
John F. Mills: No relevant relationships to disclose.
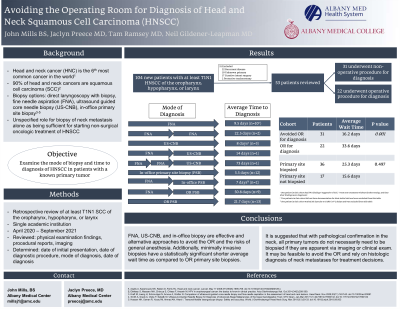
Introduction: Head and neck cancer can present with accessible pathologic lymph nodes and obtaining an adequate specimen for definitive diagnosis without direct laryngoscopy may avoid unnecessary operating room procedures. This study examines the efficiency of nonoperative procedures to establish the diagnosis and head and neck squamous cell cancer (HNSCC) in patients with clear evidence of a primary tumor.
Methods: Patient charts were reviewed retrospectively for at least T1N1 squamous cell cancer (SCC) of the oropharynx, hypopharynx, or larynx at a single academic institution between April 2020 and September 2021. Encounter notes including, physical examination findings, procedural reports, and imaging were reviewed for each patient. The mode of diagnosis for each patient was determined and wait time from initial presentation to date of diagnostic procedure was recorded.
Results: A total of 104 patients with at least T1N1 SCC of the oropharynx, hypopharynx, or larynx were identified, with 53 meeting inclusion criteria of non-surgical treatment for their disease. Thirty-one out of the 53 patients (58.5%) avoided going to the operating room for definitive diagnosis of SCC, while twenty-two (41.5%) went to the operating room for diagnosis. Of the patients who avoided the operating room, twelve (38.7%) were diagnosed by fine needle aspiration (FNA), five (16.1%) were diagnosed by ultrasound-guided core needle biopsy (US-CNB), and fourteen (45.2%) were diagnosed with an in-office primary site biopsy.
Conclusions: FNA and US-CNB offers utility to diagnose HNSCC in patients presenting with pathologic neck masses. In-office biopsy of a primary tumor is also an effective and alternative approach to avoid the risks of general anesthesia. Procedures performed outside of the operating room for diagnosis are most optimal in patients that have co-morbidities and may not require surgical treatment. Our findings suggest that with pathological confirmation in the neck, all primary tumors do not necessarily need to be biopsied if they are apparent via radiographic imaging or clinical exam.