Assistant Professor PGIMER Chandigarh, Chandigarh, India
Disclosure(s):
Gyanaranjan Nayak, MBBS MS DNB: No relevant relationships to disclose.
Introduction: First branchial cleft account for less than 8% of all branchial cleft anomalies. . They are often misdiagnosed and mismanaged due to its diverse clinical presentation and diagnostic challenges. The systematic elaboration of the clinical presentation, diagnosis, and optimal treatment of first branchial cleft anomaly Work type II (Collaural fistula) is lacking. In the present series, we have described our experience in the management of four cases of first branchial cleft fistula/sinus.
Methods: The data from 4 cases of Branchial cleft anomalies diagnosed between August 2021 to September 2022 at Post Graduate Institute of Medical Education and Research were retrospectively reviewed. All the cases underwent transparotid exploration and excision of the tract after identification of the facial nerve and its relation with the tract.
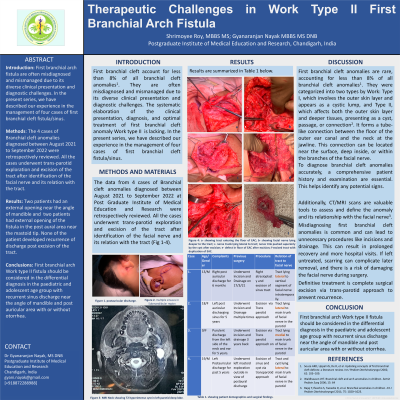
Results: The youngest patient was 9 years and the oldest was 19 years. The average duration of disease was 4 years. Two patients had an external opening near the angle of mandible and were treated with multiple courses of antibiotics. Two patients had external opening of the fistula in the post aural area near the mastoid tip and were treated with multiple courses of antibiotics at primary health care centre in the suspicion of recurrent chronic otitis media. One patient had First branchial cyst along with tract pushing the facial nerve superiorly and medially. 3 patients had internal opening of the fistula in the external auditory canal floor with ear discharge and one patient had internal opening in a blind cartilaginous sac lying just below the main external auditory canal. None of the patient has recurrence of discharge post excision of the tract.
Conclusions: First branchial arch Work type II fistula should be considered in the differential diagnosis in the paediatric and adolescent age group with recurrent sinus discharge near the angle of mandible and post auricular area with or without otorrhea.